Get the free dap notes cheat sheet form
Show details
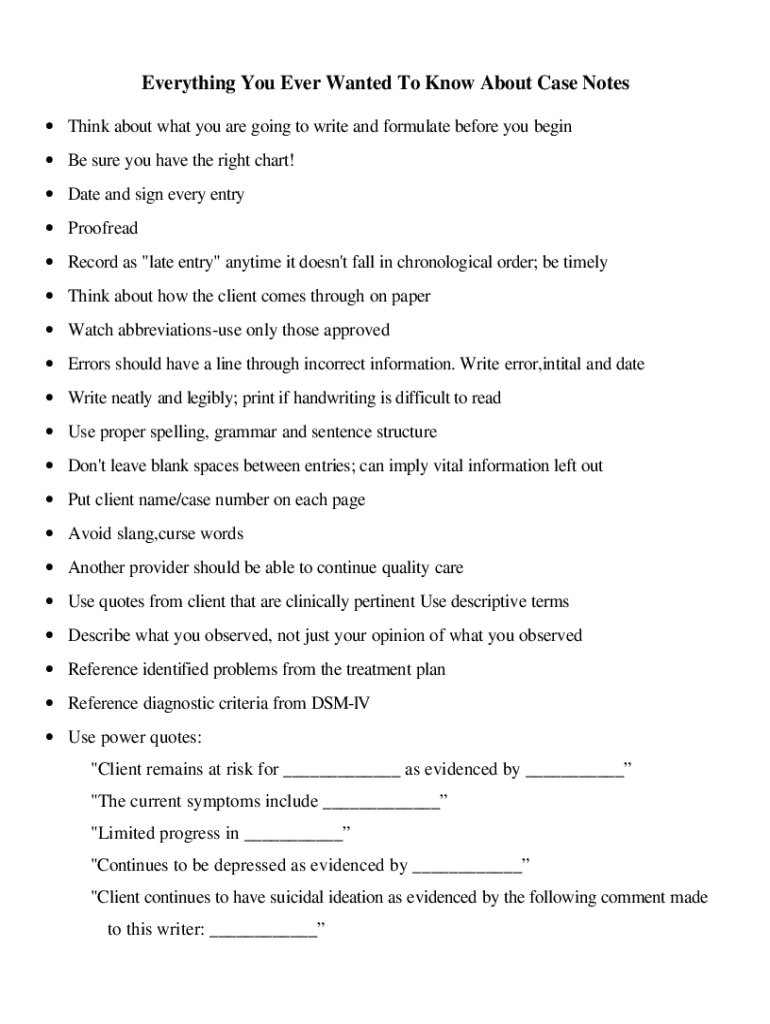
CASE NOTE FORMAT - DAP CHARTING D - Subjective and objective data about the client Subjective - what client can say or feel Objective - observable behavioral by therapist Standard I sentence progress on presenting problem review of HW Description of both the content and process of the session A - Intervention assessment -what s going on Working hypotheses gut hunches Depression appears improved this week more resistant. less involved*. P - Response or revision What you re going to do about it...
We are not affiliated with any brand or entity on this form
Get, Create, Make and Sign
Edit your dap notes cheat sheet form online
Type text, complete fillable fields, insert images, highlight or blackout data for discretion, add comments, and more.
Add your legally-binding signature
Draw or type your signature, upload a signature image, or capture it with your digital camera.
Share your form instantly
Email, fax, or share your dap notes cheat sheet form via URL. You can also download, print, or export forms to your preferred cloud storage service.
How to edit dap notes cheat sheet online



Use the instructions below to start using our professional PDF editor:
1
Log in. Click Start Free Trial and create a profile if necessary.
2
Prepare a file. Use the Add New button to start a new project. Then, using your device, upload your file to the system by importing it from internal mail, the cloud, or adding its URL.
3
Edit note format dap. Rearrange and rotate pages, add new and changed texts, add new objects, and use other useful tools. When you're done, click Done. You can use the Documents tab to merge, split, lock, or unlock your files.
4
Save your file. Select it from your list of records. Then, move your cursor to the right toolbar and choose one of the exporting options. You can save it in multiple formats, download it as a PDF, send it by email, or store it in the cloud, among other things.
pdfFiller makes working with documents easier than you could ever imagine. Register for an account and see for yourself!
How to fill out dap notes cheat sheet
How to fill out note format dap:
01
Start by writing the date at the top of the note.
02
Begin with a heading that describes the purpose or topic of the note.
03
Use bullet points or numbered lists to organize your thoughts and information.
04
Include clear and concise sentences or phrases that summarize key points or ideas.
05
Use subheadings or headings to divide different sections or topics within the note.
06
Leave ample space between each point to enhance readability and neatness.
07
Close the note with a summary or conclusion if necessary.
08
Review and proofread your note for any errors or missing information before finalizing it.
Who needs note format dap:
01
Students who wish to effectively organize their study notes or lecture summaries.
02
Professionals who attend meetings or conferences and need to document important discussions or presentations.
03
Individuals who want to maintain a systematic record of their thoughts, ideas, or research findings.
Video instructions and help with filling out and completing dap notes cheat sheet
Instructions and Help about note dap form
Hi I’m Jean Sturgeon and I create forms and other tools that make mental health counselors work easier. By the end of this brief presentation on SOAP Note Writing tips you will take away these three things: The #1 thing to remember when writing SOAP Notes A common mistake counselors make in writing notes How to help keep yourself out of legal trouble Before we begin you should know that forms do not have been a necessary evil. They can and should be a dynamic guide that leads you and your clients successfully through the therapeutic process. These SOAP note tips will help you to really appreciate the need for a quality SOAP Note form. Well let’s get started… The #1 thing to remember when sitting down to write your SOAP notes is who is your audience. Ask yourself, “Who will be reading this note?” “Who is the audience?” A SOAP Note becomes part of the client’s chart, which is the medical record. The therapist may keep therapy notes a part from the chart, but the SOAP note we are talking about today is part of the record which means it could potentially be viewed now or in the future by: The client, other professionals working with client, a judge or attorney A very common mistake counselors make is not using a concise format when writing their notes and not being intimately familiar enough with the SOAP format to remain ethically, legally and professionally above board. Here’s a takeaway: Frequently review tips on how to write a good SOAP note. I don’t know about you, but I always had trouble remembering what the acronym stands for and means. Let’s quickly review what SOAP stands for, and I’ll give you a simple example to help you understand and remember the meaning of each letter: Remember the S stands for subjective. Subjective data are typically things the client reported to you, “I am feeling very tired today and had trouble getting out of bed.” Subjective refers to data that are more like opinion. Statements colored by perceptions, feelings and experiences. The O stands for Objective. Things you the therapist observed about the client. Objective data is measurable and observable. The client kept closing their eyes and their head was nodding. Medication was increased 1 week prior. The refers to Assessment. Your professional assessment based on what was reported and what you observed in the session, “Client appears to be over medicated.” The P refers to the Plan. The plan is the action you and the client will take. In this case call a family member to drive client home. Contact the clients MD immediately to discuss symptoms and plan. Can you see how using and being familiar with the SOAP format will help you stay focused on what is important? Here’s another take away tip: Before each session review your SOAP from the previous session. During the session review the key points from your note with your client. By doing this the SOAP format drives the treatment forward. You can also see how using your SOAP note format provides the therapist and...
Fill dap format note : Try Risk Free
People Also Ask about dap notes cheat sheet
What do you write in a DAP note assessment?
How do I create a DAP note?
What is a DAP note?
What is the difference between DAP and SOAP notes?
What is the difference between DAP notes and SOAP notes?
What do you write in a DAP note assessment?
What are DAP notes for nursing?
What goes in each section of a DAP note?
What is the difference between a SOAP note and a DAP note?
What should be included in the data section of a DAP note?
Our user reviews speak for themselves
Read more or give pdfFiller a try to experience the benefits for yourself
For pdfFiller’s FAQs
Below is a list of the most common customer questions. If you can’t find an answer to your question, please don’t hesitate to reach out to us.
What is the purpose of note format dap?
Note format DAP (Documentation Aided Processing) is an organizational system used to standardize the documentation process of a project. This system helps to ensure that documents are consistent and organized, making them easier to access and interpret. The goal of this system is to provide a uniform structure for the collection and management of project documentation, allowing for efficient communication between project stakeholders and greater clarity in project outcomes.
What information must be reported on note format dap?
Note format DAP (Daily Activity Report) must include the following information:
1. Date of Report
2. Name of individual submitting the report
3. Description of the activities completed that day
4. Hours worked
5. List of tasks completed
6. Any materials used
7. Any tools used
8. Any products shipped or received
9. Any problems encountered and how they were addressed
10. Any additional comments or feedback
When is the deadline to file note format dap in 2023?
The deadline to file note format dap in 2023 is April 15th, 2023.
What is the penalty for the late filing of note format dap?
The penalty for the late filing of a note format DAP (Direct Acknowledgement of Payment) is a fine of up to HK$50,000.
What is note format dap?
There is no commonly known or recognized term or abbreviation "note format dap." It may refer to a specific format or style of note-taking, but without further context or information, it is difficult to determine its exact meaning.
How to fill out note format dap?
To fill out note format DAP (Data, Assessment, Plan), follow these steps:
1. Data (D): Start by documenting relevant information or observations about the patient or situation. Include specific details such as the patient's name, age, gender, medical history, reason for the visit, symptoms, vital signs, test results, and any other pertinent information.
Example: "Patient: John Doe, 45-year-old male with a history of diabetes. Chief complaint: abdominal pain (7/10 intensity) for the past three days. Vital signs: temperature 99.2°F, blood pressure 130/80 mmHg, pulse 80 bpm. Lab results: elevated blood glucose level (180 mg/dL). Patient reports no recent dietary or lifestyle changes."
2. Assessment (A): Analyze the data and provide an assessment of the patient's condition or situation. This includes identifying potential causes, interpreting test results, considering differential diagnoses, and summarizing the overall assessment based on the information available.
Example: "Based on the provided data, the patient's abdominal pain seems to be related to his poorly controlled diabetes. This could be due to hyperglycemia causing nerve damage in the abdomen. The elevated blood glucose level supports this conclusion. We will also consider other possible causes such as gastrointestinal issues or appendicitis."
3. Plan (P): Develop a plan of action to address the patient's needs. This should include short-term and long-term goals, treatment options, interventions, medications, referrals, or any other necessary steps. Be sure to consider the patient's preferences and include any special instructions or precautions.
Example: "The plan is to initiate immediate pain management using analgesics and to start an insulin regimen to better control the patient's blood glucose levels. Additionally, we will refer the patient to a gastroenterologist for further evaluation of the abdominal pain. The patient will also receive education on diabetes management, including diet modifications, exercise, and monitoring blood sugar levels. A follow-up appointment will be scheduled in two weeks to assess the effectiveness of the current plan and to adjust the treatment if necessary."
Remember, note format DAP is just one approach to documenting patient encounters or clinical situations. It is important to follow any specific guidelines or formats provided by your healthcare institution or practice.
Where do I find dap notes cheat sheet?
The premium pdfFiller subscription gives you access to over 25M fillable templates that you can download, fill out, print, and sign. The library has state-specific note format dap and other forms. Find the template you need and change it using powerful tools.
How do I execute note format dap sample online?
With pdfFiller, you may easily complete and sign dap note online. It lets you modify original PDF material, highlight, blackout, erase, and write text anywhere on a page, legally eSign your document, and do a lot more. Create a free account to handle professional papers online.
How can I edit dap note cheat sheet pdf on a smartphone?
The pdfFiller apps for iOS and Android smartphones are available in the Apple Store and Google Play Store. You may also get the program at https://edit-pdf-ios-android.pdffiller.com/. Open the web app, sign in, and start editing dap note generator form.
Fill out your dap notes cheat sheet online with pdfFiller!
pdfFiller is an end-to-end solution for managing, creating, and editing documents and forms in the cloud. Save time and hassle by preparing your tax forms online.
Note Format Dap Sample is not the form you're looking for?Search for another form here.
Keywords relevant to note format dap pdf
Related to dap note cheat sheet





If you believe that this page should be taken down, please follow our DMCA take down process
here
.
